Introduction
Hoarseness that lasting more than two weeks needs comprehensive ENT evaluation. The standard part of the examination is indirect laryngoscopy (1). Even for skill and well trained specialist there are some difficulties in performing this old technique (2).
The main two reasons, sometimes both present, are hyperactive gag reflex and anatomic causes of no visible larynx. The usually proposed techniques in difficult laryngeal exposure situations involve:
- use of topical anesthesia,
-some psychological and behavioral maneuvers and, finally,
- use of modern endoscopes.
On the contrary, we have chosen improving the indirect mirror examination itself.
We have already described our improvement in laryngeal mirror examination (3). Now we are presenting the results of our three years experience in performing it in everyday practice.
With this technique there is no need for topical anesthesia that is great advantage because of possible allergic reactions, some adverse effect of anesthetic for the patients, especially cough, bad taste and loose of sensitivity next few hours.
In our approach, we do not exclude use of modern instruments, of course. Furthermore, it is the only way to visualize the larynx when anatomical factors for difficult exposure are present. But if the hyperactive gag reflex is present in such situations too, our technique helps when using rigid endoscope in the office.
Fiber optic endoscope have certain limitations ( 4 ) and it can be done only after classical indirect mirror examination have been successfully performed.
Finally, direct microlaryngoscopy is the best way to recognize the reason for the hoarseness, but if indirect examination previously is well performed, there is no indication for this most expensive technique in every fifth patient, as we have shown that 18 % of such patients had no vocal pathology. .
Patients and method
During period January 2008.- December 2010. we have examined 6020 new cases of hoarseness in Phoniatric Dpt.,
There were 85 men and 47 women. Children under 11 years of age were excluded from this prospective clinical study. However it was evidenced (video documented) that the technique was successful at the age of up to five.
We have performed successful indirect laryngoscopy for 130 patients of the group.
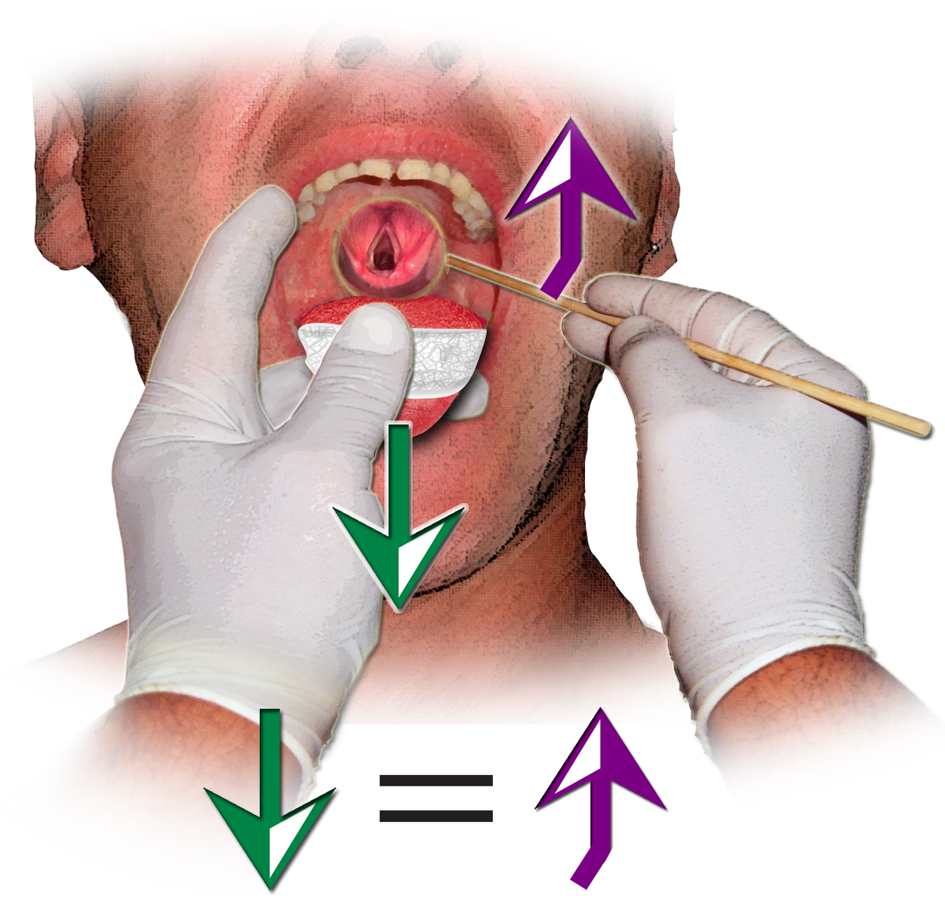
FIGURE 1- Pushing the lips corner and pulling the tongue enough strong and enough gently
If there was present hyperactive gag reflex, we have performed our maneuver with closing the patient’s nose as the essential part of the technique.
If there were some anatomical reasons for difficult larynx exposure, with or without gagging , we have performed indirect rigid laryngoscopy, with or without our maneuver.
We did not use any anesthetics.
Our clinical experience have resulted in developing some improvements that led to better diagnostic approaches more comfortable for both patient and physician. The precise description of this maneuver is shown through the Figures 1- 3. The technique is very simple, in most cases it is enough to perform indirect laryngoscopy on the classical way, but we have to emphasize the importance of same strength in opposite direction while pulling the tongue and pushing the lips corner (Figure 1) . One have to be enough hard and enough gentle, which is up to the skill and passion.
If there is hyperactive gag reflex, larynx is going up under the tongue base which makes
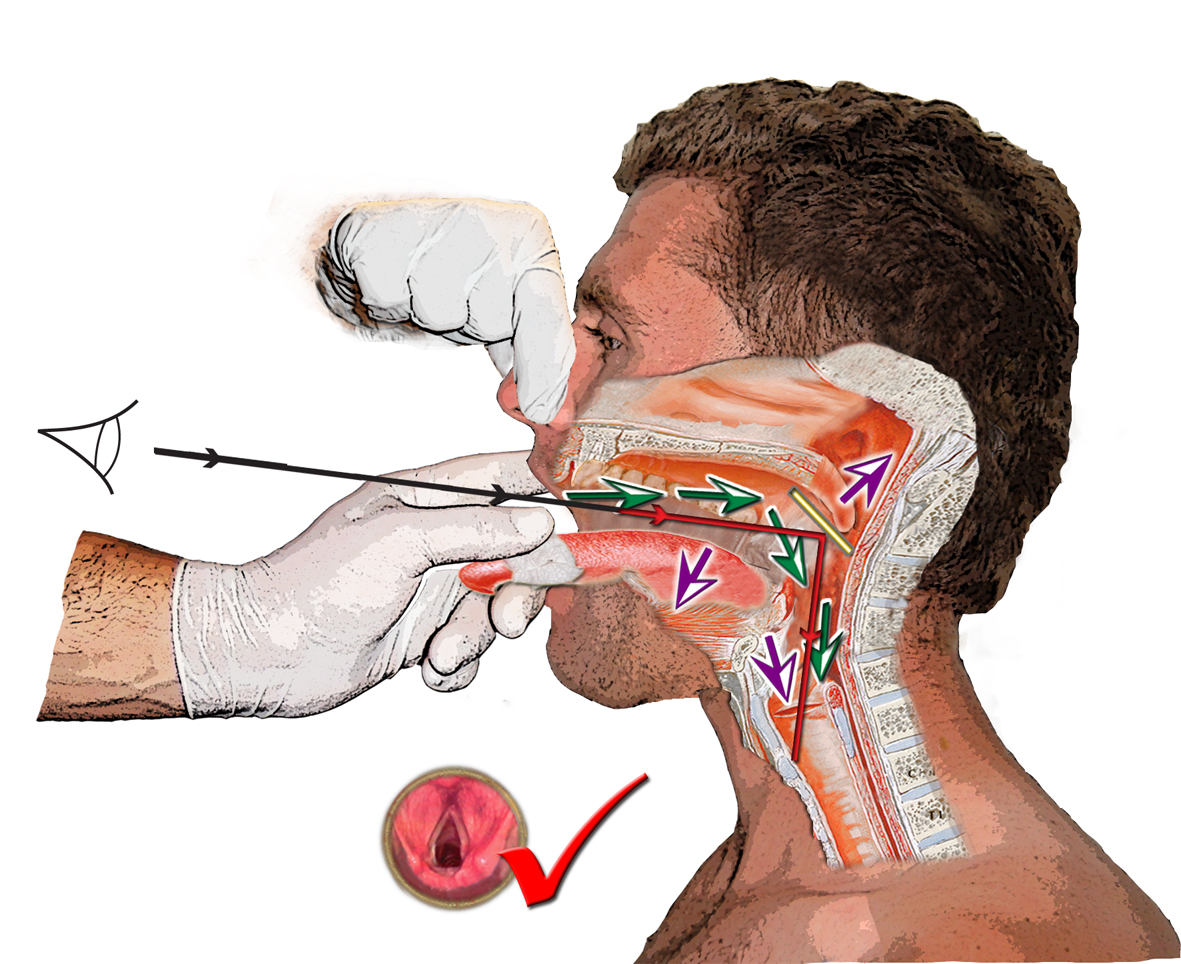
the contact with soft palate and the patient starts to breathe through the nose (one can even feel that nose breathing on index finger that is holding upper lip) , and that is the reason why the larynx becomes invisible (Figure 2). This is the essential moment of our maneuver. Just tell to the patient to breathe through the mouth, or shut his/her nose with two fingers (that can be done by patient himself or by your assistant), he will turn to mouth breathing, the gag (vomiting) reflex will disappear and the tongue base and soft palate will disconnect, and larynx will go down, enabling us to see the whole of its structures easily (Figure 3). The problem is solved.
After all, there is still possibility of not visualizing the whole larynx because of anatomic factors combined with gagging or not .The solution is examination with rigid endoscope, but performing the same maneuver, too.
We use rigid indirect endovideolaryngostroboscopy examination with the same original technique in cases of anatomical incongruence, as the reason for not visualizing the
FIGURE 2- Raising up the larynx and contact soft palate- tongue base in nose breathing while gagging , resulting with invisible larynx
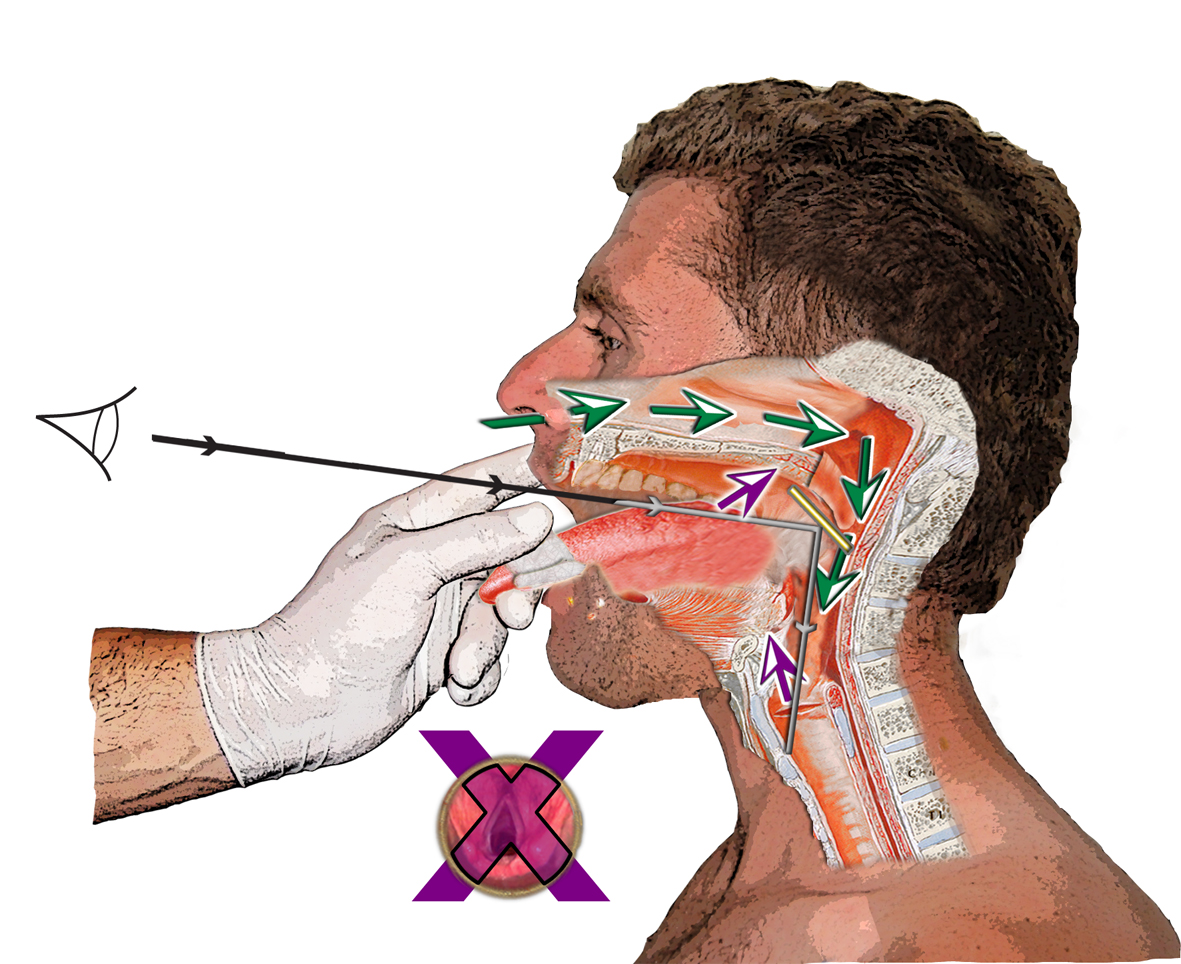
FIGURE 3- Mouth breathing after closing the nose leads to larynx going down, disconnecting tongue base and soft palate and comfortable view into the glottis
larynx with indirect laryngoscopy, and that can be done satisfactory with rigid 90 degree endostroboscope placed using the same advanced technique. We use K S Endoskope 20149920 with Telecam- C 20212034 PAL CE.
Results
Demographic parameters has given the average profile: a man, aged between 40 and 60, with hoarseness lasting for more than 6 months, physical worker, heavy smoker (surprisingly, 32 % were nonsmokers ), with no additional diseases.
The reason for such high percent of non-smokers could be loss of reflex system in nicotine damaged mucosa in smokers.
The most frequent symptom was hoarseness, unfortunately lasting more than 6 months in more than 50% of the patients. One of the reasons for such delay was fear of unpleasant examination in patient expectations, but also unsatisfactory larynx visualization in repeated examinations by ENT specialists.
It was very interesting that 16 patients had one or more previous direct microlaryngoscopies, out of whom; one had three successive procedures within the short period of time.
The fact that 18 % of patients had no organic laryngeal pathology recommends this original method as a cost effective. On the other hand, the fact that malignant pathology is evidenced in 16 % of the cases, emphasizes its importance. Furthermore, vocal fold polyps were diagnosed in 11 % , chronic laryngitis in 17 % and Reinke edema in 20 % (Table 1).
TABLE 1 Clinical findings with improved technique of larynx visualization in difficult exposure situations
|
No pathology |
23 |
|
Vocal fold carcinoma |
21 |
|
Edema Reinke |
26 |
|
Laryngitis chronic |
22 |
|
Vocal fold polyp |
14 |
|
Other pathology |
24 |
|
Total |
130 |
Successful indirect laryngoscopies were performed in 106 patients
(80 %), successful visualization with indirect rigid endovideolaryngostroboscopy, performed with the advanced technique in 24 patients (19%). There was no need for using topical anesthetics.
There were only 2 patients whose vocal folds were not seen at all, and they were sent to direct microlaryngoscopy. These were patients both with vocal fold carcinoma.
Discussion
Is it not amazing that the technique of indirect laryngoscopy remained unchanged for more than 150 years? The most frequent reason why otolaryngologists and patients run away from this old method is gag reflex as one of the most important disadvantages.
Indirect laryngoscopy, also known as laryngeal mirror examination or mirror laryngoscopy is not simple- to- perform procedure (1). Although this old fashioned method of larynx visualization was introduced two centuries ago (2), the main two objectives are still the same, gagging and anatomical factors of difficult exposure.
Anatomic factors were seen in near 20% of our patients. The most frequent are (5):
- Short, thick, fat neck
- Limited neck movement (Fused vertebrae)
- Poor palatal visualization (Lingual hypertrophy, macroglossia, tonsil hypertrophy)
- Jaw malformations (Retro and micrognathia, trismus or reduced interincisor opening)
- Dental malformations (long teeth, prosthesis, and malocclusion)
- Lingual malformations (Ankyloglossia, tongue paralysis)
- Oversize of thyroid - mandible angle
There is very clear reason why all of patients who otherwise can not make the nose breathing while their mouth is open during the epipharyngoscopy, always change to the nose breathing during indirect laryngoscopy. That is unconscious defense reaction during gag reflex development.
Hyperactive gag reflex is vomiting reflex in fact. Touching the patient’s palate with the mirror triggers the vomiting reflex. It comprises several stages:
- Deep inspire
- Rising up of hyoid bone and larynx, as well as soft palate making contact with tongue base,
- Glottal closing
Gag reflex is involuntary, defense contraction of pharyngeal and laryngeal musculature elicited when mucosal receptor recognize foreign substance presence or tactile stimulation. Trigeminal, gloss pharyngeal and vagus fibers are included in reflex arch, with sub cortical center in medulla oblongata, and some, not well defined, cortical influence.
About one-third of healthy people do not have a gag reflex (6) , although have intact pharyngeal sensation. About 15 % of patients have hypersensitive gag reflex (7).
There are very few articles in ENT literature about managing gag reflex (8, 9, 10).
Much more ENT articles, especially from the last decades of 20th century, are about advantages of modern technology comparing with indirect laryngoscopy (11).
Computed Tomography (12), Magnetic Resonance Imaging, Multidimensional Computer Analysis of Voice and Speech (13), Endovideolaryngostroboscopy (flexible or rigid) (14), etc., seem to be the most powerful diagnostic tools, as well as direct microlaryngoscopy, ultrasonic imaging and autofluorescence laryngoscopy .
Over the last decade, even more advanced tools have been developed (15): multiple- flash- timing laryngeal videostroboscopy, videostrobokymography , digital kymography, high-speed videoendoscopy, narrow band imaging (16), thresholding techniques and phonovibrogram (17), with multiple combining imaging and other analysis techniques. Surprisingly, in last decade, there are articles in which you can find that mirror laryngoscopy provides reliable diagnosis in most patients (18).
On the contrary, there are much more articles about managing hyperactive gag reflex in dentistry literature (19). Preventing the gag reflex was proposed by behavioral techniques, techniques of systematic desensitization or pharmacological techniques. Authors precisely describe that breathing through the nose is physiologically self defense part of gagging reflex, and also mention that topical anesthetics may increase nausea and vomiting in some patients.
Furthermore, using of topical anesthetics can influence vibratory patterns of the vocal folds assessing by stroboscopy.
Finally, in anesthesiologist literature there are data about this topic by describing difficult laryngeal exposure management (7). In this article we can find interesting data that 75 patients refused indirect laryngoscopy, as well as data about classification of laryngeal views in four stages and the most interesting information that indirect laryngoscopy was abandoned because of excessive gag reflex in 449 patients, even when skilled laryngoscopists were doing the examination.
In this article we have described an improvement in indirect laryngoscopy technique. Mirror examination is easy to perform in patients who do not have gag reflex and if there are no anatomical factors for difficult exposure.
In cases of hyperactive gag reflex, there is no need for topical anesthesia, it is also easy to perform it with our technique, that we strongly recommend for office based practice.
In cases of anatomical factors for invisible larynx, with or without gag reflex, the solution is indirect rigid laryngostroboscopy, performed with this maneuver . Fibernasolaryngoscopy, if it is available, is also very good solution, but only if indirect laryngoscopy is previously done, in order to evaluate anatomy and mucosal hygiene (position of the base of the tongue, lingual and pharyngeal tonsil tissue, hydration of pharynx and larynx and presence of pharyngeal pooling) (20), as well as to eliminate neglecting of possible neoplasm of oro and hypopharynx, that ca be hidden for fiberoptic instrument.
The fact that only 1% of our patients were sent to direct laryngoscopy under general anesthesia shows cost effectiveness of this technique. At the same time, in countries where modern technology is not available yet, this is solution for 80% of patients. From the point of preventive medicine view, making indirect laryngoscopy easier to tolerate, can encourage patients to seek the physician in earlier stage of their hoarseness.
Nowadays, ENT specialists, laryngologists and non-medical voice and speech therapists do not perform indirect laryngoscopy in everyday practice at all; they just use endoscope as the only tool. Certain limitations of Manuel Garcia technique cannot be the reason for such erroneous practice.
There is no alternative to classical medicine and well-established diagnostic protocols.
Modern technology has limitations not only in economic field (contemporary tools are still too expansive). Furthermore, errors (4) caused by movements of the endoscope, low spatial end temporal resolution, absence of generally accepted clinical protocols, variations in illumination and a large variability of the appearance of vocal folds, suggest that industry of modern tools will have much more job in the coming years.
Absence of skill should not be the reason for neglecting the old fashion methods in office-based practice.
Conclusion
We have presented the improvement of the method of indirect laryngoscopy that can help practitioners in visualizing vocal pathology in difficult exposure situations. We offer a protocol for larynx visualization (Table 2)
There are four stages in laryngeal exposure;
- Indirect laryngoscopy
- Endovideolaryngostroboscopy (rigid)
- Fibernasolaryngoscopy
- Direct microlaryngoscopy
Being successful in 80% of non visible larynx visualization, our technique can be helpful tool in everyday ENT practice, especially where modern instruments are not available.
We recommend this maneuver in situations of anatomical causes of difficult exposure (19% in our series) that present with or without gag reflex, when rigid endoscope is available.
Precise history and classic clinical examination are corner stones of good practice, yesterday, today and tomorrow. Advances in laryngeal imaging have an important role
TABLE 2 – Larynx visualization protocol

nowadays, but only if proper history is obtained and classical examination performed previously. We have to be fully aware of all advantages and limitations of modern technology and the classical medicine should not be neglected.
Modern technology is helpful, but only as a part of standard, step by step, well defined protocol. Absence of skill as well as modern industry offensive should not be the reasons for neglecting the technique of indirect laryngoscopy in everyday ENT practice.
Do we see the patient himself in the forest of modern instruments?
Literature
- Geza J. (1991.) Laryngeal Endoscopy and Microlaryngoscopy. In Paparella M. (ed) Otorhinolaryngology.
Philadelphia - Bailey B. (1996) Laryngoscopy and laryngoscopes- who is first?: the forefathers/ four fathers of laryngology. Laryngoscope, 106: 939- 43
- Micic D.(1998) Hoarseness. Acta Clinica/ Clinical
Center ofSerbia ,Belgrade
8 (3): 58-66
- Kotby M.N., Hassan O., El-Makhzangy Aly M.N., et al. (2010) Gastroesophageal reflux/ laryngopharyngeal reflux disease: a critical analysis of the literature. Eur Arch Otorhinolaryngol, 267 (2): 171- 9
- Pinar E., Calli C., Oncel S., et al. (2009) Preoperative clinical prediction of difficult laryngeal exposure in suspension laryngoscopy. Eur Arch Otorhinolaryngol, 266 (5): 699-703
- Davies A., Kidd D., Stone S., et al. (1995) Pharyngeal sensation and gag reflex in healthy subjects. Lancet, 345: 487- 8
- Yamamoto K., Tsubokawa T., Shibata K.et al. (1997) Predicting Difficult Intubation with Indirect Laryngoscopy. Anaesthesiology, 86(2): 316- 21
- Delclos L. (1976) Technical note: A finger extension tongue depressor. Laryngoscope, 86(3): 454- 7
- Kollar A. (1989) Indirect laryngoscopy. Cesk Otolaryngol, 38(2): 114- 5
- Draper M.r., Blagnys D., Premachandra D.J. (2007) To EE or Not to EE. J Otoralyngol, 38(3): 191- 95
- Grabas C.S., Charabi S., BalleV.H. (2001) The relevance of mirror examination in modern otorhinolaryngology.Ugeskr Laeger, 163 (47): 6586- 9
- Beser M., Erdogan G., Yener M., et al. (2009) Detection of laryngeal tumors and tumoral extension by multislice computed tomography- virtual laryngoscopy (MSCT-VL). Eur Arch Otorhinolaryngol, 266 (12): 1952- 8
- Godino-Ljorente J.I., Osma Ruiz V., Saenz-Lechon N., et al. (2008) Acoustic analysis of voice using WPCVox- a comparative study with MultiDimensional Voice Program. Eur Arch Otorhinolaryngol, 265(4): 465- 76
- Rosen
C.A. - Verikas A., Uloza V., Bacaurkiene M., et al. (2009) Advances in laryngeal imaging. Eur Arch Otorhinolarygol, 266 (10): 1510- 20
- Piazza C., Cocco D., De Benedeto L., et al. (2010): Narrow band imaging and high definition television in the assessment of laryngeal cancer: a prospective study on 279 patients. Eur Arch Otorhinolaryngol, 267 (3): 409-14
- Lohscheller J.,
Ey-boldt U. - Dunkleberger J., Rhee D., Kim S. et al. (2009) Video rigid laryngeal endoscopy compared to laryngeal mirror examination: An assessment of patient comfort and clinical visualization. The Laryngoscope, 119 (2): 269- 71
- Bassi G.S., Humphris G.M., Longman P.L. (2004) The etiology and management of gagging: A review of the literature. J Prosthet Dent, 91: 459- 67
- Woo P. (2006) Laryngeal examinations and visualizations in Benninger S.M., Murry T. (ed) The Performers Voice, Plural Publishing,
San Diego
