Conservative Treatment vs Phonosurgery
___________________________________________
Abstract
In our Phoniatric Dpt. everyday practice we try to keep specific multidisciplinary approach to the communication disorders, that includes an expert team using modern technology.
Over the last six years we have treated 110 singers ( 3% of all new cases) and the results of their diagnostic and therapeutic management are presented here. There were 67 women and 43 men, 41 were smokers and 69 nonsmokers. The singing genres included 24 pop, 41 folk, 8 ethnic, 29 choral and 8 opera singers. The therapy success was compared with the demographic parameters, level of education and music genres across the subjects.
A precise history, clinical examination, endovideolaryngostroboscopy and multidimensional computer analysis of voice and speech was carried out by two phoniatricians, two logopeds, two nurses and one clinical psychologist. Additional consultations were carried out by audiologists, allergists, endocrinologists, chest physicians, gastroenterologists and neurologists where necessary.
We suggest that the gold standard is conservative therapy, with phonosurgery if conservative measures fail.
We also suggest that an annual systematic examination is optimal in preventing disease in professional singers.
Key words: multidisciplinary approach, annual systematic examination
NOTE- This is modified version of Free Paper Presentation on “Choice for Voice 2008 “ Conference, that was hold in London, on July, 10th – 12th
Introduction
At our current level of understanding, the voice is a specific human acoustic phenomenon, produced by highly synchronized coordinated activity in the multiple systems involved between the acoustic apparatus and voice production. The history is half the diagnosis. Some of the very important history factors include the working conditions, duration of the work experience, nicotine or alcohol dependency, use of illicit drugs and other underlying medical conditions. The onset of the symptoms and their relationship to vocal activity is also important.
Otorhinolaryngologic examination should include examination of the ears for disease or malfunction, nasal function, movement of the tongue and soft palate, the larynx and the cervical spine for the neck disorders. Attention is given to the type and rhythm of respiration and the presence of nasal or oral breathing.
Phoniatric examination provides information about the presence of hyperkinetic voice production, such as hard vocal attack in speech. Psychoacoustic analyses are made of intensity, frequency, perturbation, maximal phonation time, intonation and prosody.
To become an expert phonosurgeron requires good psycho physiologic insight, combined with the ability to recognize the smallest details, to be extremely precise and to work in three dimensions. Extensive knowledge of vocal physiology and pathology is essential. Occasionally, in spite of skilled surgical and anaesthetic staff, good instrumentation, and precise phonosurgical techniques, some patients are not completely satisfied with the result of microsurgery. One explanation is that distortion in phonatory coordination disturbed the vocal function resulting in organic pathology. In these cases phoniatric rehabilitation is the key of the management. The first and most important step is to make the correct diagnosis.
Videostrobolaryngoscopy is a very important tool when evaluating the need for endolaryngeal microsurgery. If there is symmetry and regularity of the vocal fold vibrations, whatever the pathology, the gold standard therapeutic approach is conservative treatment.
It is important to mention that there is no way of making a clear differential diagnosis between so called organic and functional lesions. Perfect microsurgical ablation can be performed on vocal nodules, but it will still be necessary to deal with the residual hyperkinetic vocal production, which can lead to the formation of nodular changes again and again. During rehabilitation, the inefficient voice production patterns must be fundamentally changed and the new efficient patterns stabilized so that they become automatic. It is important to see the whole person with a holistic medical, psychological and professional approach before making a decision about therapy. Any additional disturbances need to be recognized in order to achieve the optimal situation in the laryngeal mucosa for the rehabilitation.
Multidimensional computer analysis of the voice and speech is one of the best diagnostic tools that also serves well to evaluate the success of rehabilitation. It can also be used as documentation for the clinical, scientific, educative or forensic purposes.
Method
Each patient had an initial detailed phoniatric interview and a later “control” one. The control interview allows a second chance to re-evaluate the problem where the patient may give some additional information, and the physician may notice additional symptoms or signs. Every patient had a complex otorhinolaryngologic and phoniatric examination with psychoacoustic analysis of the voice. All patients received videolaryngostroboscopy and multidimensional computer analysis of their voice and speech, as well as evaluation of the musicality of their voice.
We are currently using the commercial Dr Speech programme (2004) for the multidimensional computer analysis. This includes - Real Analysis, Vocal Assessment with Electroglottograph, Phonetogram for the full musical range, and a Scope View.
In ambient noise of less than 50 dB a microphone type CM 903 Electret Condenser Meeting Microphone (with Pre Amplifier T/ 11) was used. The mouth to microphone distance was calibrated and standardized for each participant and the whole 5 sec signal was analyzed from the optimal trial.
A prolonged /a/ vowel was used in the voice analysis (pronounced as the English letter R).
Speech analysis was carried out using originally formed sentences and standardized text made and presented in cooperation with the Electrotechnic Institute and Philology Institute. These standardized texts provide the best phonetic and syntactic representation of the Serbian language.
The Phonetogram testing of the musical range was carried out using the standardized protocol formed in 1981 at the UEP Congress in
Videostroboscopy was carried out using an Endoscope with camera (Telecam- C 20212034 PAL CE) and installed microphone, with the usual endoscopic and advanced stroboscopic light ( Karl Storz endoscope 20140020).
When necessary, we requested additional evaluations for the following areas: audiology, psychology, bacteriology, radiography, allergy, pulmonary, neurology, endocrinology and gastroenterology.
To optimize the rehabilitation of the laryngeal mucosa, a multimodal therapeutic approach was adopted which included inhalation therapy, nasal decongestion and specific treatment for any additional disease, including supportive psychotherapy.
Where microsurgery was indicated, individually planned preoperative and postoperative rehabilitation was provided.
A multidisciplinary approach was used with every patient. The Scope View and other computer assisted programs documentation were used for documentation and also as an educational tool for patients and students.
Phoniatric rehabilitation was used as the gold standard for each patient.
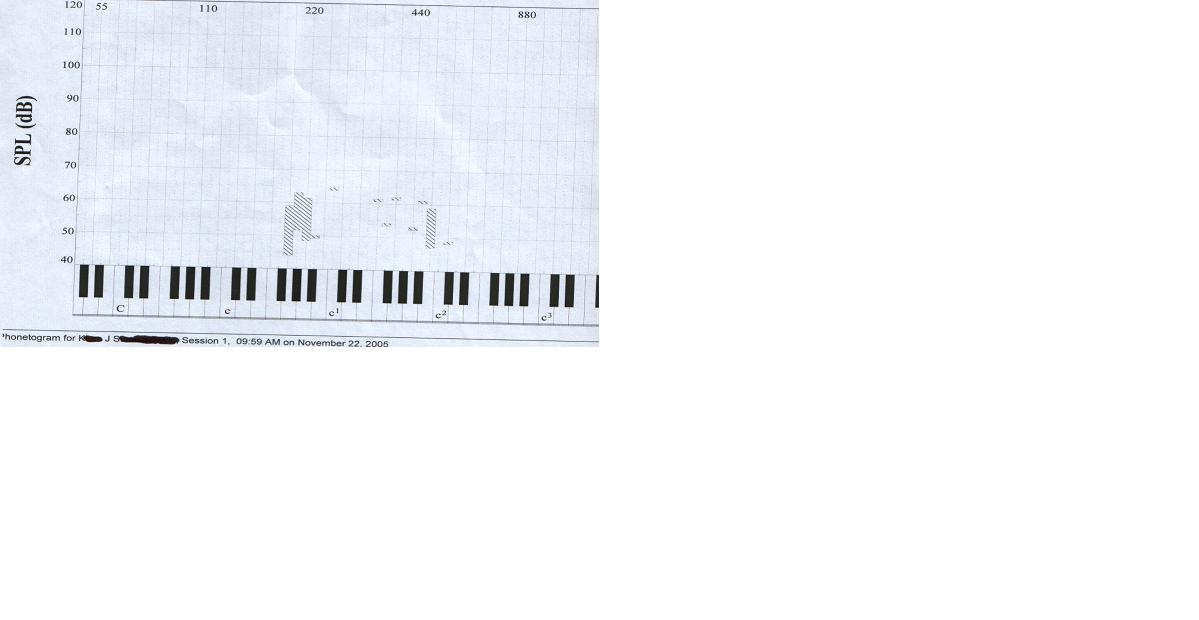
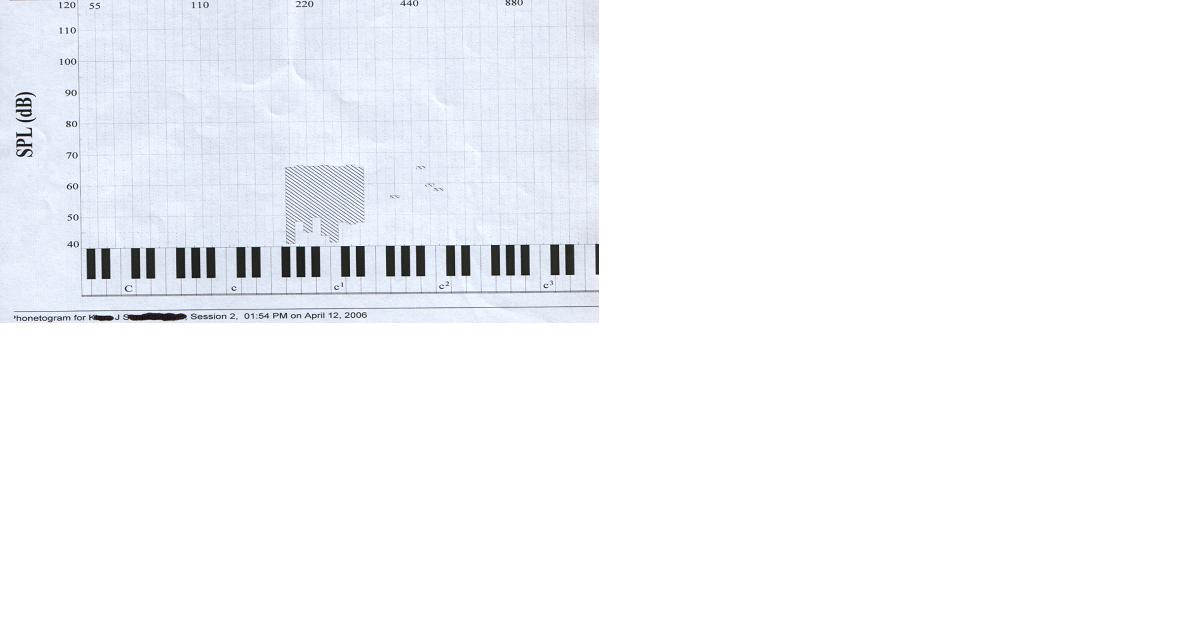
FIGURE 1 - Phonetogram of Reinke edema voice before and after the conservative treatment
The first step was to optimize the status of laryngeal mucosa with medications such as inhalations, decongestants, anti allergy therapy, proton pump inhibitors, etc together with a very consistent anti smoking management.
Our maxim is that surgery is the last step of the treatment. Where necessary a limited phonomicrosurgery is performed, always keeping in mind the necessity to preserve enough tissue for adequate vocal fold vibrations.
Lesions affecting the vocal fold mass such as nodules are treated conservatively without surgery. Polyps are mostly removed surgically with the firm rule that the micro instruments are used in only a “forward- backward” way.
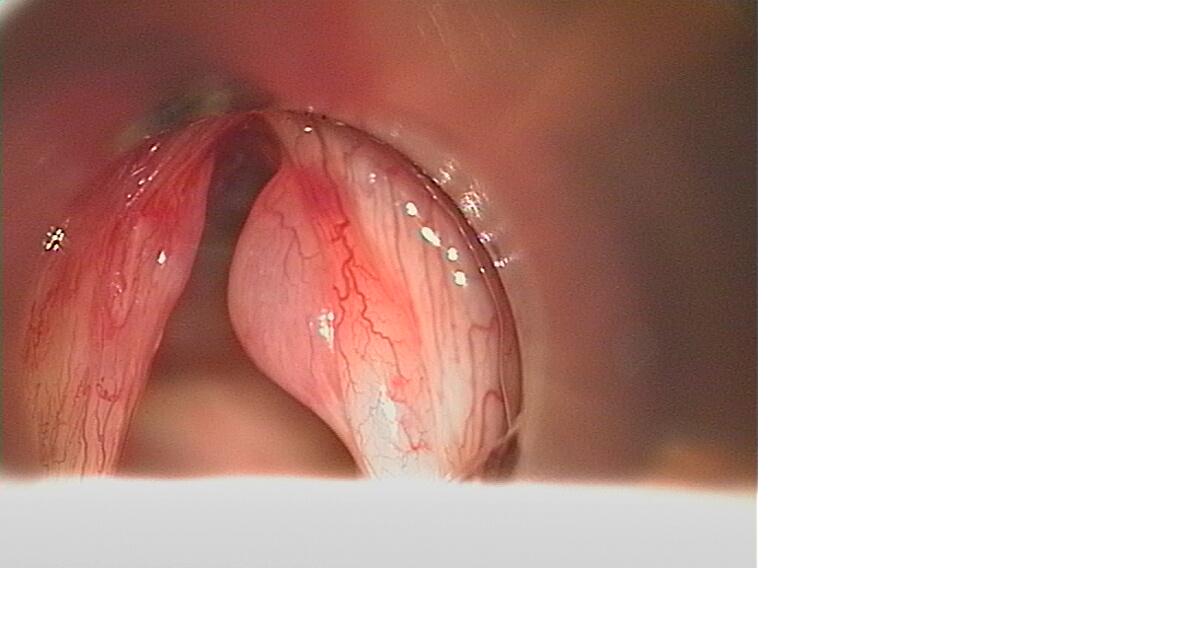
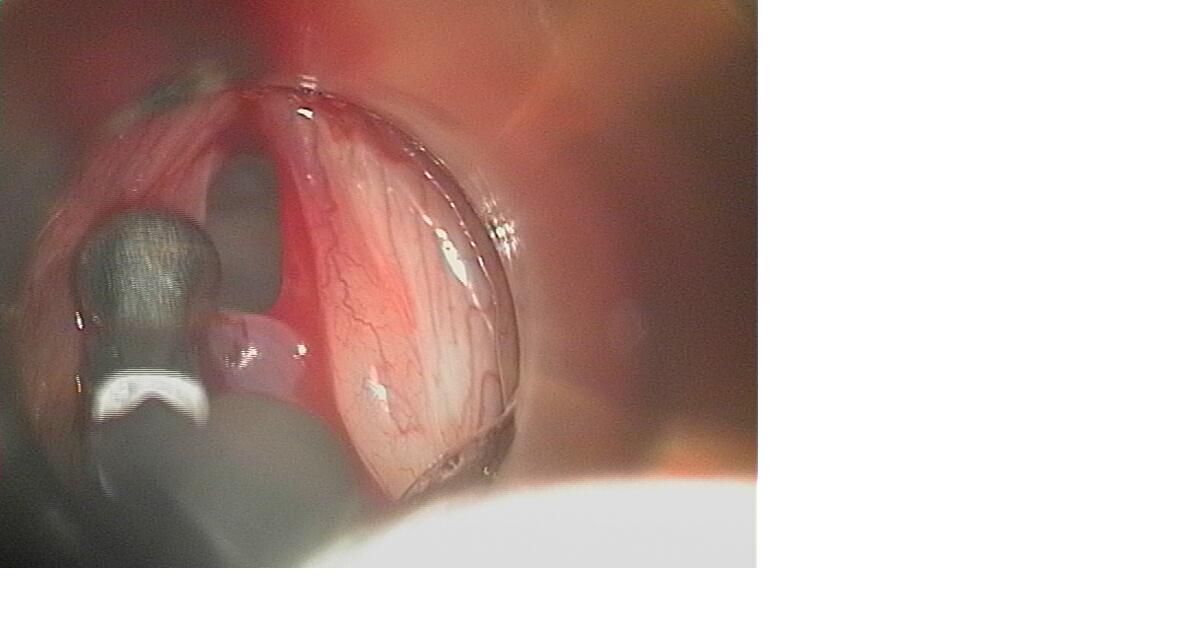
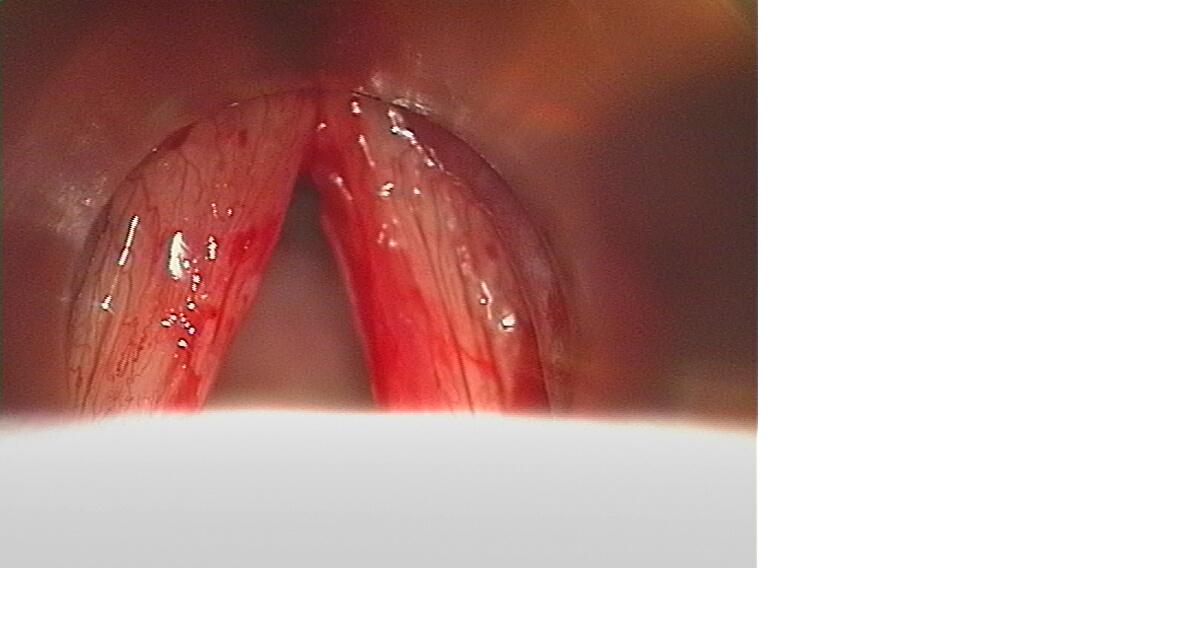
FIGURE 2 - Obvious forward- backward move
Patients with Reinke edema stages II and III are treated with incision and aspiration so that eventually the redundant mucosa stabilizes. Cysts are for micro preparation. Contact ulcers, sulcus and haematoma are managed with conservative treatment.
Results and discussion
In a prospective clinical trial over the last 6 years we cared for 110 professional singers.
67 of them were women and 43 of them were men.
61 were aged between 21- 30 years, 23 were aged between 31-40, 15 were aged between 41- 50, and 11 were aged between 51- 60 years old.
67 had been singing for between 1-10 years, 31 had been singing for between 11- 25 years, and 12 had been singing for between 26- 40 years.
There were 41 smokers, and 69 nonsmokers.
24 of the group were pop singers, 41 were folk singers, 8 sang in an ethnic genre, 29 were choral singers, and there were 8 opera singers.
64 had no singing educated, 18 had a primary level of music education, 17 had reached secondary musical education and 11 had reached a high level of music education.
Among the 46 with a singing education, there were 33 soprano voices, 4 altos, 3 tenors and 6 basses.
Hoarseness was the predominant symptom in uneducated group, and dysodia (disturbance of the singing voice) was the predominant symptom in educated group, especially in the group with a high level of the education. We can assume that there is confusion about terminology in the uneducated population, and that the term hoarseness is used for every case of voice problems.
Some singers do not attend to their voice problem for economic reasons. The nature of the music markets means that they will often wait until the voice problem becomes severe before seeking treatment to avoid loss of income. There is also the issue of high environmental noise in the uneducated group that can hide voice problems during singing for a longer time.
The fact that 47 in the group of 64 uneducated singers did not seek advice until their illness had lasted longer then 2 months is consistent with the previous explanation. Anecdotally, one of them had experienced hoarseness for 30 years.
We can also conclude that among the educated group the sopranos appeared to be the most worried about their voices. 20 of the 33 sopranos went to the phoniatrician within two months of their presenting symptoms, 7 of them in first two weeks.
We could see that the uneducated singers had the most serious diagnoses. There was relatively high level of vocal nodules among sopranos with primary music school education, and the relatively high level of chronic rhinopharygitis among sopranos with middle and higher levels of musical education (6 with middle, and 5 with the higher level of music education). Rationale can be discussed, but from a psychosomatic viewpoint, the likelihood is that sopranos are the most sensible singer population.
Table 1- Distribution of the therapy mode and success compared with the educational level
|
Therapy mode and success |
Un-educated |
Pri mary |
|
|
|
Middle |
|
|
|
High |
|
|
|
|
|
|
S |
A |
T |
B |
S |
A |
T |
B |
S |
A |
T |
B |
|
Conserv. success |
47 |
9 |
1 |
3 |
2 |
13 |
1 |
|
2 |
10 |
|
|
1 |
|
Conserv. fail |
3 |
1 |
1 |
|
|
|
1 |
|
|
|
|
|
|
|
Surgery success |
6 |
|
|
|
1 |
|
|
|
|
|
|
|
|
|
Surgery fail |
8 |
|
|
|
|
|
|
|
|
|
|
|
|
In Table 1 we can see the distribution of the therapy mode compared with the educational level
Our conservative therapy is successful, especially with the educated singers (only one went on to require surgery). The uneducated group is also successful as shown by the success rate of 47 out of 50 conservative treatments. 2 of the 4 altos failed with conservative treatment. Finally we can conclude that surgery is not a successful therapy option for singers (8 failures of 15 surgical treatments).
Successful treatment signifies that the singer continues to do his job after the treatment.
We could see that symptoms like pain, postnasal secretion and voice change are reserved for nonsmokers, aged 21- 30, and mostly women.
Less experienced, younger women, mostly nonsmokers showed relative prompt need for medical help.
In our work we confirmed the well known fact that polyps and chronic laryngitis are most commonly found in men, and Reinke edema and vocal nodules are more commonly found among women. It also demonstrates that rhinopharyngitis with associated allergy was more commonly seen in females.
Polyps, Reinke edema, chronic laryngitis are associated with smoking.
Vocal nodules are more often found in the younger population.
Anecdotally, we have seen one singer aged 21, who had a 6 year experience of heavy smoking.
Table 2- Distribution of the therapy success compared with demographic parameters
|
Therapy success |
Years |
Of |
exp |
Sm |
oke |
A |
g |
e |
|
Gen |
Der |
|
|
1-10 |
11-25 |
26-40 |
Yes |
No |
21-30 |
31-40 |
41-50 |
51-60 |
M |
F |
|
Conserv. success |
58 |
23 |
8 |
27 |
62 |
56 |
16 |
9 |
8 |
34 |
55 |
|
Conserv. |
3 |
1 |
2 |
5 |
1 |
2 |
2 |
|
2 |
1 |
5 |
|
failure |
|
|
|
|
|
|
|
|
|
|
|
|
Surgery success |
2 |
3 |
2 |
4 |
3 |
1 |
3 |
2 |
1 |
4 |
3 |
|
Surgery failure |
4 |
4 |
|
7 |
1 |
2 |
2 |
4 |
|
4 |
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
In Table 2 we can see distribution of therapy success compared with demographic parameters
Conservative therapy is successful in nonsmokers, and conservative therapy and surgery more likely to fail in smokers.
Choral and opera singers recognize the problems in their singing voice, while pop and rock singers recognize hoarseness as the first symptom. We also need to re-evaluate the widespread opinion that certain aspects of hoarseness are often considered a positive feature in the voices of pop and rock singers.
Diagnoses such as polyp, Reinke edema and chronic laryngitis are mostly made in pop and folk singers. The fact that rhinopharyngitis associated with allergy was mainly diagnosed in choral and opera singers, is also interesting. We postulate that it may be related to stage dust.
No patient in this study had a diagnosis of contact granuloma, laryngeal nerve paralysis or malignancy.
Table 3- Distribution of therapy success compared with music genre
|
Therapy success |
Pop |
Folk |
Ethnic |
Choral |
Opera |
|
Conserv. success |
18 |
29 |
8 |
26 |
8 |
|
Conserv. |
1 |
2 |
|
3 |
|
|
failure |
|
|
|
|
|
|
Surgery success |
3 |
4 |
|
|
|
|
Surgery failure |
2 |
6 |
|
|
|
In Table 3 we can compare therapy success with the music genre
The pop and folk singers who had surgery as the final step of their treatment were unfortunately mostly failures rather than successes. Failure is understood as being unable to continue with their job. Fortunately, in general, singing was not their only way of making a living.
- our view, singers who ask for help and advice when they are ill, in spite of an upcoming performance, are rare. Those who take the advice of their physician seriously are rare indeed. Most are seeking a quick resolution of their immediate problem, usually with ‘miracle’ medicaments, regardless of the consequences tomorrow. In many cases, the physician has to make a compromise. We advise the performer to sing anyway if he or she must do so, but to undertake absolute vocal rest in all other daily circumstances such as general conversation, laughing, coughing, phone calls etc. Aerosol corticosteroids are a part of such compromise, but with the serious caveat that performing under such circumstances may be dangerous for their career and should not be repeated. Should this situation occur again it may be wise to suggest the singer finds another doctor. We also always advise that they consult their voice teacher.
Anecdotally, we have seen one successful jazz and blues singer with 30 years of experience followed by a break of 10 years. Having decided to return to performance, she made a visit to the physician. This is a further example of how this group of professionals are interesting and complex individuals
Conclusions
In our experience, most singers are very sensitive human beings, who are worried about their instrument, but without the knowledge as to how to protect it. The important factor is musical education; there are numerous musically uneducated or self educated singers in our population. The most important factor is health education; the singer must keep his/her voice, (the most perfect instrument), better than the musician keeps his violin. Vocal hygiene should be a subject in music school, especially with a focus on antismoking behavior. There must be the closest cooperation between music schools of all levels and The Voice Centre (Phoniatric Department, or Communication Disorders Care Centre etc.) There should be annual systematic examinations for every student, initially when they are first accepted, to exclude vocal pathology, and subsequently every two years to ensure their continuing vocal health. There should also be similar systematic examination among the professionals throughout their careers. We cannot stress enough the importance of screening examinations for this population. Abnormal findings have been reported in up to 58% of healthy, asymptomatic professional singers (Elias, Sataloff, Rosen, 1997). Furthermore, if the performer has annual systematic reports, any change in evaluation will be a “red light” for the need for intervention.
The minimum protocol should consist of otorhinolaryngologic and phoniatric examination, including audiometric, videolaryngostroboscopy, multidimensional computer analysis and, if there is any sign of disease, additional pulmonary, endocrine, allergy, neurological and gastroenterological analysis.
Only multimodal, interdisciplinary management can help the dysphonic patient, especially if he is a professional singer. The key is to reinstitute phonatory coordination. We must influence the patient to stop overuse or inefficient use of the voice and move him out of bad environmental circumstances. An aggressive and effective anti smoking campaign is important and we should identify and minimize risk factors for every individual. We must make a plan for every patient, but a plan which will incorporate a standard protocol. We must give stable psychological support and avoid overuse of medication, especially considering the well known tendency of singers to take `”anything that will help just for tonight”.
The best phoniatrician should be a singer, too.
The eternal question in medicine is what is the primary problem? Is it organic or functional? This question has its place here too. Is there a functional disorder if a patient is dysphonic after microsurgery, and we cannot find any visible organic cause? Is it an organic disorder if a patient has dysphonia after microsurgery, and we can see relapse of the mass on vocal fold? In most cases, diagnostic and therapeutic decisions tend to be made depending on the findings at the first interview, although there may be complex development of the disease later. There is a temptation to deal with the organic problem rather than its functional cause. The only reasonable way forward is always to deal with both in the management of every case. We must think about the patient and not about the disease.
Literature
1. Altman KW, Atkinson C, Layarus C. Current and emerging concepts in muscle tension dysphonia: a 30 months review. J Voice 2005; 19: 261- 7
2. Behrman A., Sulica L. Voice rest after microlaryngoscopy: current opinion and practice. The Laryngoscope 2003; 113: 2182- 6
3. Benninger S.M., Murry T. The Performers Voice. Plural Publishing,
4. Gerhard F., Remacle M., Birchall M., et al. Defining phonosurgery: a proposal for classification and nomenclature by the Phonosurgery Committee of the ELS. Eur Arch Otorhinolaryngol 2007; 264: 1191- 1200
5. Hanania NA, Chapman KR, Kesten S. Adverse effects of inhaled corticosteroids. Am J Med 1995; 98: 196- 208
6. Hansen JK, Thibeault SL. Current understanding and review of the literature:vocal fold scarring. J Voice 2006; 20:110- 20
7. Johns M.M. Update on the etiology, diagnosis and treatment of vocal fold nodules, polyps, and cysts. Curr Opin otolaryngol Head Neck Surg 2003; 11:456- 61
8. Kaszuba MS., Garret G. Strobovideolaryngoscopy and laboratory voice evaluation. Otolaryngol Clin N Am 2007; 40: 991- 1002
9. Kilic MA, Ogut F., Dursun G., et al. The efects of vowels on voice perturbation measures. J Voice 2004; 18: 318- 24
10. Klein A.M., Johns M.M. Vocal Emergencies. Otolarygol Clin N Am 2007; 40: 1063- 80
11. Neely JL., Rosen C. Vocal fold hemorrhage associated with coumadin therapy in an opera singer. J Voice 2000; 14: 272- 7
12. Rubin AD., Praneetvatakul V., Heman- Ackah Y., et al. Repetitive phonatory tasks for identifying vocal fold paresis. J Voice 2005; 19: 679- 86
13. Sataloff T.R., Hawkshaw J.M. Voice Surgery. Otolaryngol Clin N Am 2007; 40: 1151- 83
14. Sama A, Carding P.M., Price S., et al. The clinical features of functional dysphonia. Laryngoscope 2001; 111: 458- 63
15. Sherer RC.,Rubin JS. Laryngeal physiology: normal and disordered. In: Benninger MS, ed. Benign Disorders of Voice .
16. Schneider SL., Sataloff TR. Voice therapy for the professional voice. Otolaryngol Clin N Am 2007; 40: 1133- 50
17. Treole K., Trudeau MD. Changes in sustained production tasks among women with bilateral vocal nodules before and after voice therapy. J Voice 1997; 11 (4); 462- 9
18. Woo P. Office Based Laryngeal Surgery. Otolaryngol Clin N Am 2006; 39: 111- 34
19. Yang Y., Lewis JD, Epstein S., et al. Long term proton pump inhibitor therapy and risk of hip fracture. JAMA 2006; 296 (24): 2947- 53
20. Yhang Y., Jiang JJ. Chaotic vibrations of a vocal fold model with a unilateral polyp. J Acoust Soc Am 2004; 115 (3): 1266- 9
